The Oversimplification of Tackling Loneliness in Social Prescribing
30th Sep, 2022
My Loneliness Is Killing Me: The Oversimplification of Tackling Loneliness in Social Prescribing
HOW LONELINESS HARMS US
HOW LONELINESS HARMS US
Loneliness is a subjective emotional state. The Cognitive Discrepancy Theory of Loneliness describes it as dissatisfaction with the discrepancy between one’s desired and actual quality and quantity of social relationships. It is therefore a perceived, rather than objective, social isolation.
Loneliness has been suggested to be associated with negative health outcomes such as reducing our immunity against infections by reducing the number of natural killer cells we have1, and elevating our risk of earlier mortality by up to 26%2. The lack of sense of belongingness that is often felt with loneliness is one of the biggest risk factors for suicide3. Social prescribing schemes have therefore been implemented, aiming to reduce loneliness and improve psychological and physical wellbeing. These schemes involve healthcare professionals referring people to link workers for support. Link workers will then refer them to suitable non-clinical local community programmes, such as befriending schemes, volunteering, and shared activity and group learning programmes.
But do these schemes really work to reduce loneliness? Reducing objective social isolation, by increasing the number of social contacts a person has, does not necessarily reduce loneliness, as the two don’t always correlate. For example, one study found that those who felt lonely in 2004 were more likely to be depressed 12 years later, and that their experience of subjective loneliness was not related to their age, social class, health, or social activities4. Crucially therefore, the relationship persisted in those who were not objectively socially isolated. Due to loneliness’ subjective nature, some people may feel content with many ‘superficial’ friendships, whereas for someone else one deeply trusted friend may be all they need to satisfy them. Are these schemes able to target the wide variety of experiences of loneliness that people feel?
In this blog, I will discuss whether group-based social prescribing schemes alone can reduce subjective loneliness and improve health outcomes, whether it views tackling loneliness in an overly idealistic manner, and if our focus should be on addressing the cognitive processes behind loneliness instead.
DEFINING AND MEASURING LONELINESS
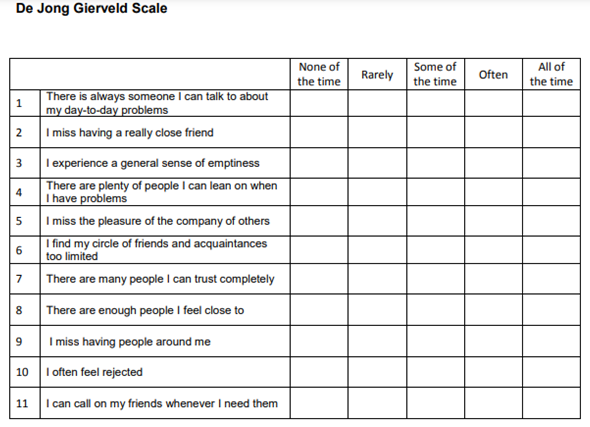
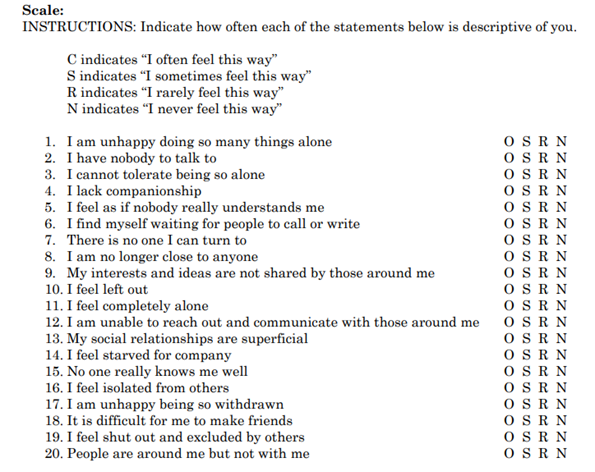
The highly personal and subjective nature of loneliness makes it hard to define. This raises the question of how loneliness can be measured in research effectively to evaluate the therapeutic benefit of social prescribing interventions. Common loneliness scales used in research are the UCLA Scale5 [Figure 1] and De Jong Gierveld Scale6 (DJG) [Figure 2]. The DJG Scale splits loneliness into two parameters: social loneliness, the subjective lack of desired quantity of relationships, and emotional loneliness, the lack of desired quality and meaningfulness of relationships. There is some evidence that these scales can provide an accurate estimate of loneliness, with the DJG Scale correlating with loneliness-related risk variables from other studies6. Furthermore, one study on different measurements of loneliness using data from 31 countries found that even single item measurements of loneliness had high correlation with other measurements for quantifying loneliness in the same countries, as well as meaningful correlation of variation in scores on different scales across countries7.
However, it may be worth noting that the UCLA and DJG scales are indirect measures of loneliness, in that neither explicitly mention “loneliness” in them, rather asking questions related to the concept of loneliness. But if loneliness is so subjective, it could be argued that asking someone directly how lonely they feel on a visual analogue scale of 0-10 would be a better qualifier, as one could interpret what loneliness means for them personallyand answer based on that. It could be argued that this could capture the subjective nature of loneliness more, however this still highlights the difficulty of quantifying loneliness as this would also likely not provide generalisable results as baseline scores could mean something different if everyone interprets loneliness with a different meaning. Another flaw of the current scales used is that loneliness is not a static state of being, like any emotional state it fluctuates, but these questionnaires only provide a measure of an individual’s loneliness at one snapshot in time. Therefore, it may be more effective to analyse changes in scores from these scales over a period of time.
The validity of these loneliness questionnaires is of even greater importance when it is considered that loneliness data, including risk stratification, is often used to predict where the loneliest individuals live and to therefore identify eligible people for social prescribing schemes. The use of these scales, if invalid, could therefore prevent those who most need the services from accessing them. Psychological barriers also prevent lonely people from accessing social prescribing schemes. There are links between loneliness, anxiety, and depression, with lonely people experiencing high levels of social anxiety8, meaning people suffering from mental health disorders and loneliness may lack motivation or energy to join and engage with services that may be of help to them.
THE POTENTIAL HARM OF SOCIAL PRESCRIBING INITIATIVES AIMING TO TACKLE LONELINESS
Is it possible that social prescribing schemes aiming to reduce loneliness could do more harm than good? The effects of social prescribing on tackling loneliness have not been greatly evaluated, as most studies evaluating this are pilot studies. It has been noted that there is a lack of good-quality evidence regarding social prescribing’s impact on wellbeing, with poorly designed studies, high risk of bias, lack of comparative controls, and short follow-up durations9 10. One systematic review failed to show that there was a causal relationship between reported changes in loneliness following social prescribing interventions9, with another review concluding that there is little evidence of the effectiveness of social prescribing schemes due to the poor quality data available11. Similarly, another systematic review of 9 trials reported that whilst participants felt less lonely and more connected to others after social prescribing interventions, the studies were of low quality with limited pre/post study design or control group comparisons meaning the generalisability of the results is uncertain11. As discussed, the validity of the loneliness scale’s used in these studies also complicates the interpretation of their findings. For example, despite one study finding that patients reported better scores on patient reported outcome measures after social prescribing interventions compared to before, whether these differences are clinically significant and therefore meaningful to patients depends on the validity of the loneliness measurements used12. A flaw of this study was the use of independent observations rather than individual paired comparisons for the evaluation of PROM scores before and after social prescribing. Therefore, there is a need for more high-quality studies into the impacts of social prescribing on loneliness to accurately evaluate its effectiveness.
“Improving the quality of relationships and increasing companionship, meaningful connections, and providing a sense of belonging, should be a key part of these strategies. It is not sufficient just to increase the time spent with others.”4
Increasing a sense of belongingness has been suggested to be important in reducing feelings of loneliness3 13. One study showed that when participants were asked to remember a time they gained a ‘low-esteem group identity’, meaning when they joined a group that is stigmatised by others, they reported experiencing lower life satisfaction, self-esteem and greater depressive symptoms than losing a group identity, suggesting that in some cases, joining a group can be more harmful than losing a group identity14. People could view community support and health groups as ‘low-esteem groups’, and experience these negative effects on wellbeing. The degree to which people feel like they belong in a group and are similar to its other members affects the extent to which the group influences a person’s concept of themselves, which is thought to play in a role in how much benefit is gained from therapy groups15. This principle underlies ‘social cure effect’ theory of groups, which proposes that to obtain psychological need satisfaction from being a member of a group, the membership must be perceived by the individual as meaningful and important16. This theory also highlights the importance of whether the group provides social support, particularly from people the individual identifies with.
One study of people with neurological conditions who were involved in social prescribing schemes noted that many felt obliged to join groups despite experiencing high levels of anxiety and feeling like they were not benefiting from them8. Conversely, among those who were optimistic about joining groups, it was not uncommon for them to report feeling lonelier and more alienated once they had joined them compared to before. They attributed this to failings on their own behalf: saying that social-anxiety and low self-esteem prevented them from connecting with the group. There are suggestions that lonely people are highly vigilant to negative social cues during social interactions, anticipating rejection and therefore developing negative social biases17. These negative cognitive biases could reduce the potential therapeutic benefit they could receive from social prescribing schemes. Therefore, this may create a self-fulfilling prophecy where patients anticipate rejection and feel like they are not going to fit in with the groups, increasing their anxiety and impacting their ability to engage and interact with the groups and gain any potential benefits. This is supported by the finding that lonely people can approach social encounters with cynicism and mistrust, adopting behaviours that are paradoxically more likely to increase their chance of rejection18. As previously discussed, simply increasing the number of social contacts people have is not enough to reduce feelings of loneliness. But if someone is led to believe that joining a group will help them feel less lonely, and it doesn’t, they may think the problem lies within them and like it is a failing and weakness on their own behalf that they haven’t felt able to fit in with the groups or gain any benefit, and this could lower their self-esteem even further. Could it be better to tackle cognitive biases associated with loneliness to enable people to engage fully with these groups, as opposed to putting them in groups they may not be psychologically ready to face, which could end up doing harm?
Two studies analysing different loneliness interventions have found that psychological approaches to address ‘maladaptive social cognition’, focussing on adapting how people think about social relationships, provided the greatest benefit over interventions that increased social skills, social support, and number of social contacts19 20. It is possible therefore that the greatest synergistic benefit may be seen by targeting cognitive processes first with psychological therapies to address underlying cognitive biases and reasons why people feel lonely, followed by then increasing the number of social contacts to provide an environment where they can put what they learnt through the psychological therapy into practice. An approach to this could be to screen individuals for negative cognitive biases so that those who need more support get individualised care for this, whilst those who are ready to join a group can do so.
Improving people’s ability to connect with their community would also likely improve their health. With the closure of communal spaces such as pubs and village halls, there is less opportunity for people to interact21. It would be hard for someone to rebuild their social network when access to these community spaces is lost. This links to criticisms made of social prescribing ‘over—medicalising’ our lives, in that people now must see a health care professional to attend groups that were previously part of a normal society. Therefore, it is important to support funding for initiatives and policies like place-based approaches, which identify issues in communities and tackle them to try and reduce geographical inequalities in health, such as increasing the number of green spaces, social places and community events, and Big Society and Healthy New Town initiatives which included aims to help prevent local facilities and services from closing22 23. Whilst these approaches may not be able to tackle serious cases of loneliness alone, they may help reduce the number of people who feel lonely to begin with.
CONCLUSION
Whilst social prescribing interventions to tackle loneliness provide a promising move in the right direction given loneliness’ association with health outcomes, there is an urgent need for better quality research surrounding which interventions can provide the most benefit. Due to the possible cognitive biases present in those experiencing loneliness causing them to anticipate rejection from recalling past negative social experiences, it is possible that increasing the number of social contacts someone has by introducing them to community groups may cause more harm than good, and solidify their pre-existing biases. Therefore, it may be that psychological interventions targeting individuals’ biases and social anxieties should be the first-line intervention provided by social prescribing to reduce loneliness. Loneliness is an inherently personal and subjective emotional state, and there is therefore great difficulty in defining it and evaluating the impact of current interventions on it. The lack of clinical assessment tools and clinician awareness of the health association with loneliness means medications are often prescribed, whilst discussions to support reconnecting may be more valuable. Regardless, the severity of the need to tackle the prevalence of loneliness to improve people’s psychological and physical wellbeing is clear. It is likely that due to the personal nature of loneliness, one intervention will not be the best fit for all. Clear communication and discussion with patients about what loneliness means to them and what intervention may best suit their needs is needed when discussing social prescribing schemes, as to avoid any potential adverse effects of allocating them to an unsuitable scheme.
REFERENCES
- Kiecolt-Glaser, J. K. et al. Psychosocial modifiers of immunocompetence in medical students. Psychosom Med 46, 7-14 (1984).
- Holt-Lunstad, J., Smith, T. B., Baker, M., Harris, T. & Stephenson, D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspect Psychol Sci 10, 227-237 (2015).
- Calati, R. et al. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. Journal of Affective Disorders 245, 653-667 (2019).
- Lee, S. L. et al. The association between loneliness and depressive symptoms among adults aged 50 years and older: a 12-year population-based cohort study. The Lancet Psychiatry 8, 48-57 (2021).
- Russell, D., Peplau, L. A. & Ferguson, M. L. Developing a measure of loneliness. J Pers Assess 42, 290-294 (1978).
- De Jong Gierveld, J. & Van Tilburg, T. The De Jong Gierveld short scales for emotional and social loneliness: tested on data from 7 countries in the UN generations and gender surveys. Eur J Ageing 7, 121-130 (2010).
- Newmyer, L., Verdery, A. M., Margolis, R. & Pessin, L. Measuring Older Adult Loneliness Across Countries. The Journals of Gerontology: Series B 76, 1408-1414 (2021).
- Simpson, S., Furlong, M. & Giebel, C. Exploring the enablers and barriers to social prescribing for people living with long-term neurological conditions: a focus group investigation. BMC Health Serv Res 21, 1230-1230 (2021).
- Vidovic, D., Reinhardt, G. Y. & Hammerton, C. Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. Int J Environ Res Public Health 18 (2021).
- Bickerdike, L., Booth, A., Wilson, P. M., Farley, K. & Wright, K. Social prescribing: less rhetoric and more reality. A systematic review of the evidence. BMJ Open 7, e013384 (2017).
- Reinhardt, G. Y., Vidovic, D. & Hammerton, C. Understanding loneliness: a systematic review of the impact of social prescribing initiatives on loneliness. Perspect Public Health 141, 204-213 (2021).
- Benson, T., Seers, H., Webb, N. & McMahon, P. Development of social contact and loneliness measures with validation in social prescribing. BMJ Open Quality 10, e001306 (2021).
- Kellezi, B. et al. The social cure of social prescribing: a mixed-methods study on the benefits of social connectedness on quality and effectiveness of care provision. BMJ Open 9, e033137 (2019).
- DeMarco, T. C. & Newheiser, A.-K. When groups do not cure: Group esteem moderates the social cure effect. European Journal of Social Psychology 49, 1421-1438 (2019).
- Cruwys, T. et al. Predictors of social identification in group therapy. Psychother Res 30, 348-361 (2020).
- Häusser, J. A., Junker, N. M. & van Dick, R. The how and the when of the social cure: A conceptual model of group- and individual-level mechanisms linking social identity to health and well-being. European Journal of Social Psychology 50, 721-732 (2020).
- NIHR. Loneliness is strongly linked to depression among older adults, a long-term study suggests,
- Hawkley, L. C. & Cacioppo, J. T. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med 40, 218-227 (2010).
- Mann, F. et al. A life less lonely: the state of the art in interventions to reduce loneliness in people with mental health problems. Soc Psychiatry Psychiatr Epidemiol 52, 627-638 (2017).
- Masi, C. M., Chen, H.-Y., Hawkley, L. C. & Cacioppo, J. T. A meta-analysis of interventions to reduce loneliness. Pers Soc Psychol Rev 15, 219-266 (2011).
- Harris, J. Britain’s shared spaces are vanishing, leaving us a nation of cliques. The Guardian (2018).
- McGowan, V. J. et al. Examining the effectiveness of place-based interventions to improve public health and reduce health inequalities: an umbrella review. BMC Public Health 21, 1888 (2021).
- Fund, P. H. E. T. K. s. Putting Health into Place: Executive Summary. (2019).